8.1 Donor blood testing
All donors have testing for transmissible infectious diseases and for organ allocation. Blood is taken from potential donors, sometimes before family agreement to donation, and transported to Auckland. The bloods will only be tested after family agreement to donation. This practice facilitates donation in a timely manner and reduces the distress for families that can be associated with long waiting periods before the commencement of the donor surgery.
All donors have the following infectious disease testing:
- hepatitis B and C
- HIV
- syphilis
- human T-lymphotropic virus (HTLV)
- cytomegalovirus (CMV).
Testing for organ allocation includes:
- ABO and Rh blood grouping
- HLA typing and transplant crossmatching.
These tests are completed at the New Zealand Blood Service (NZBS) in Auckland. It is important for the Donor Blood Pack to be transported to Auckland as early as possible so that testing commences as soon as family consent has been given. The testing takes about 6 hours and the donor surgical team(s) will not travel to the donor hospital until these results are available.
Plasma dilution
Plasma dilution by intravenous fluids may lead to false negative infectious serology results. Calculation of plasma dilution is carried out by the donor coordinator. The calculation determines whether the sample taken for infectious serology testing is suitable to be tested, otherwise there is a risk of false negative results due to the dilution of the sample.
The donor coordinator requires information about all intravenous fluid (blood, colloid and crystalloid including pre-hospital) administered during the 48 hours prior to the blood samples being taken. If plasma dilution is significant the donor coordinator will request a pre-dilution sample from the laboratory, if it is available.
The donor coordinator will ask the ICU to include this sample in the Donor Blood Pack.
Donor Blood Pack
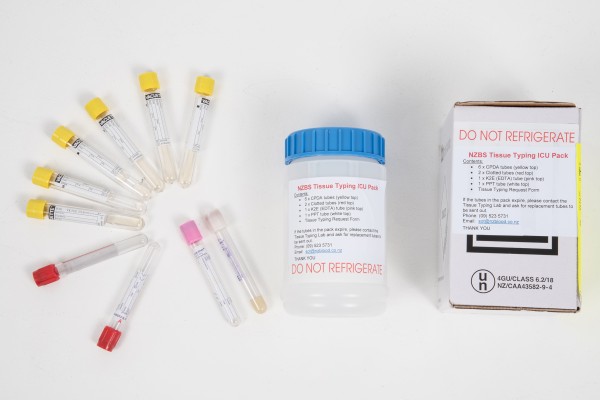
There is a Donor Blood Pack available in every ICU. It includes:
- outer cardboard box
- screw top plastic container
- 7 x 10ml CPDA (yellow top) Tissue Typing tubes
- 2 x 6ml clotted (red top) tubes
- 1 x 6ml K2E EDTA (pink top) tube
- 1 x 5ml PPT (white top) tube
- laboratory form.
The pink tube for ABO and Rh blood grouping must be handwritten. Patient stickers can be used for all other tubes and the laboratory form.
Place the completed form and blood tubes in the plastic container and then inside the cardboard box for transport. The donor coordinator will arrange transport of the Donor Blood Pack from your ICU to Auckland.
NZBS will automatically send a replacement Donor Blood Pack. If you need a new Donor Blood Pack or the blood tubes have expired, please email the donor coordinator: [email protected]
Paediatric donors
If there is concern about the volume of blood required, please contact the donor coordinator.
For some blood groups a smaller volume of blood might be possible. The mother of neonates and breast-fed children will also need to be tested for infectious diseases.
8.2 COVID-19
All donors should be screened for COVID-19 by both:
- history of risk factors and
- laboratory testing (as advised by ODNZ).
ODNZ requires that the screening by history of risk factors conforms to the most recent recommendations from the Ministry of Health.
Active COVID-19 does not exclude donation. If a donor tests positive for COVID-19 further information may be required by the transplant services.
8.3 Coronial consent
The Coroners Act 2006 defines the circumstances where a death must be referred to the coroner. When the coroner accepts jurisdiction over the death, the coroner will determine the cause of death and issue a death certificate.
In cases where the coroner accepts jurisdiction, the removal of organs and tissues cannot proceed without the agreement of the coroner.
The coroner’s agreement is obtained by the ICU doctor. Most commonly this takes place after determination of brain death. In DCD, provisional agreement from the coroner must be obtained before death (and before intensive therapies are withdrawn). The Coroners Act only empowers the coroner to make decisions after the death of a person. However, the Chief Coroner has agreed that in circumstances of potential DCD, waiting for Coronial agreement until after the death is impossible and that provisional agreement prior to the death can be given.
Organ donation can occur with coronial agreement in circumstances of possible homicide. ODNZ recommends that organ donation be discussed with the family in these circumstances as the coroner is required to consider the family’s views.
However, the family should be informed that the coroner may legally withhold agreement.
In making a decision about organ donation, the coroner may seek advice from the forensic pathologist and the police. The ICU doctor should enquire if the coroner requires any additional information that might be of help.
There are a number of options which might enable both organ donation and the needs of the coroner, the forensic pathologist and the police, to be met. These include:
- bedside clinical examination of the patient by the forensic pathologist prior to organ donor surgery
- attendance by the forensic pathologist at the donor surgery
- CT scanning prior to donor surgery
- tissue biopsies taken during donor surgery
- formal report by donor surgeons of operative findings.
ODNZ can assist with exploring these options.
Identification of the patient
In all cases where the coroner has accepted jurisdiction, the police must be notified and the patient formally identified by the family. This should be done before the family leaves the hospital.
If the police arrive to identify the patient after brain death while the patient is still ventilated, the ICU staff must be available to explain brain death to them, if needed.
In the circumstance of DCD, formal identification by the family will usually take place after the donor surgery. The timing of this can be immediately afterward, if the family is present, or at a later time if they have left the hospital.
There may be situations where identification can take place prior to withdrawal of intensive therapies. This will require the assistance and understanding of the police involved.
8.4 Information required by the donor coordinator
Accurate information is required about the potential donor to enable the transplant teams and tissue banks to determine suitability of the organs and tissues for transplantation.
| Donor Blood Pack |
|
| Useful early information |
For potential DCD:
|
| Stage of donation process |
|
| COVID-19 testing |
|
| Information required for all patients (DBD and DCD) |
History and current clinical assessment:
Medications:
Laboratory results from admission to day of referral, investigations:
|
| Potential heart donor ≤ 65 years (DBD only) |
|
| Potential pancreas donor ≤ 45 years (DBD only) |
|
| Potential lung donor ≤ 75 years (DBD or DCD) |
|
| Potential kidney (DBD or DCD) |
|
| Documentation to be emailed to the donor coordinator | The following documentation should be emailed to the donor coordinator [email protected]:
|
8.5 Medical/Social Questionnaire
It is important to obtain accurate information about the patient being considered for donation.
The donor coordinator will ask the ICU staff to complete the Medical/Social Questionnaire with the family. This questionnaire helps to determine the risk of disease transmission from the donor to the recipient(s) through transplantation.
The Medical/Social Questionnaire asks about the patient’s general health information, risk of having acquired a transmissible disease though overseas travel and includes sensitive questions in relation to sexual behaviour, drug use and other matters.
It is important to complete the questionnaire with the person(s) with the best knowledge of the patient’s past medical and social history.
Due to the sensitive nature of some questions, it is advisable to complete this questionnaire in a private room away from other family members or friends.
If the person does not know the answer to a question, they should be asked if there is another person who you or the donor coordinator can get this information from, eg a friend or their general practitioner.
If the answer to a question is unknown, please discuss with the donor coordinator.
All questions answered with a Yes require further questions to establish exact information. For example, if there is a history of heart disease, they should be asked what it was, when it was diagnosed and what treatment he/she had received since diagnosis.
The completed questionnaire is emailed to ODNZ at [email protected].
Click here to download the Medical/Social Questionnaire
8.6 Driver licence information
In May 1999, the question “Would you be willing to donate organs in the event of your death? Yes/No” became compulsory before obtaining a New Zealand driver licence. It is asked again when the licence is renewed every 10 years. If the response is “Yes”, the word DONOR is printed on the licence.
The question is asked at a time when the main purpose is to obtain a driver licence and full and accurate information about organ donation is not provided. It does not meet usual requirements for “informed consent”.
For some people a “No” arises from a strongly held and informed position, but others may say “No” because they think that they are too old or unsuitable to donate organs or tissues.
In New Zealand, driver licence information is not routinely accessed before donation is discussed with the family.
The Human Tissue Act 2008 requires both informed consent and a lack of informed objection before donation can occur. The Act states explicitly that the driver licence information does not constitute informed consent or objection.
The driver licence information is not binding on the family and a decision about donation is still theirs to make.
Some families believe that it will be reassuring for them to find out the driver licence information. There should be a discussion with the family about how this information will affect their decision, especially if it is contrary to their views.
If the family wants this information, it can be obtained by the donor coordinator who will require the patient’s full name, date of birth and current address.
8.7 Donor family support
Confidentiality for donor families and recipients
Confidentiality is maintained for the protection of the donor family and the recipients and their families.
The donor family is informed of the recipient in general terms, if they wish to receive that information, eg “the heart was transplanted to a middle-aged man”.
This information is shared with families one to two weeks after the donation.
Follow-up and support by the donor coordinator
The donor coordinator meets with the family before the donor surgery, if the family is present and wishes to meet. For many families it can be reassuring for them to meet the donor coordinator who will be present with their family member during the donor surgery. The donor coordinator discusses with the family the follow-up that can be provided and answers any questions the family might have.
Some families wish to receive a phone call from the donor coordinator at the completion of the donor surgery or the following day to let them know the outcome of donation.
One to two weeks following the donation, the donor coordinator writes a letter of thanks to the family on behalf of the transplant teams, the recipients and their families. This letter includes general information about the recipients unless the family has indicated that they did not wish to receive such information.
Written information on brain death, the process of organ donation and bereavement are sent with this initial correspondence to the family.
The donor coordinator phones the family six to eight weeks after the donation to offer further information and support. Ongoing follow-up for some families can be for many years.
Handprints and locks of hair
The donor coordinator offers to take handprints and locks of hair for the family. These are sent to the family with the initial correspondence.
Anonymous correspondence between donor families and recipients
Some recipients wish to thank the family by writing a personal letter of thanks, which they do anonymously. This correspondence is passed on through the donor coordinator, if the donor family wishes to receive it. Donor families sometimes write to the recipients and this is handled in the same way.
Thanksgiving services
Thanksgiving services are held annually for donor families, recipients and health professionals. These services respectfully acknowledge the generosity of families who have donated organs and tissues for transplantation.